

Background: Hematologic malignancies arise in the 5th through 7th decades of life resulting in the need for aggressive treatment in an aging population with inherent comorbidities. We previously reported on the efficacy of a myeloablative two-step haploidentical hematopoietic stem cell transplant (HI HSCT). Herein, we report the results of our prospective trial utilizing a reduced intensity conditioning (RIC) HI-HSCT two-step platform in older patients.
Methods: The RIC regimen consisted of fludarabine, thiotepa (33%) OR busulfan (67%), and 2 Gy total body irradiation (TBI). An unmanipulated donor lymphocyte infusion (DLI) containing 2 x 108/kg T cells was infused three days after the completion of the conditioning regimen. Two days later, cyclophosphamide (CY) was administered for bidirectional tolerization of the donor lymphocytes, followed one day later by a CD34 selected stem cell infusion. In the current clinical trial, three rest days were added between the completion of the conditioning regimen and the administration of the DLI. We hypothesized that the extra days would allow further conditioning-related tumor burden reduction, less alloreactive tumor-specific T cells activation and thus avoid eradication by CY. Patients were enrolled from 2013-2020. Due to higher than expected non-relapse mortality (NRM), the protocol was amended in 2015 to require that patients age ≤ 60 years have ≤5 HCT-CI points and KPS ≥ 80%, age 60-65 have ≤4 HCT-CI points and KPS ≥80%, age 65-69 have ≤3 HCT-CI points and KPS ≥90%, and ≥ 70 have ≤2 HCT CI points and ≥KPS 90%. The study was approved by the Jefferson IRB and all subjects were consented according to the Declaration of Helsinki.
Results: Forty-two patients with AML (14), MDS (7), Hodgkin Disease (5), myeloproliferative disorder (4), multiple myeloma (3), diffuse large cell lymphoma (3), mantle cell lymphoma (2), CMML (1), Ph+ ALL (1), T cell NHL (1), and marginal zone lymphoma (1), were treated from 2013 to 2020. Median age and KPS were 60 (range 22-74) years and 90% (range 80%-100%) respectively. At a median follow-up of 42 (range 2-78) months, the 2-year probability of survival (OS) was 41%, and cumulative incidence (CI) of relapse and NRM were 23% and 41%. CI of acute and chronic GVHD were 44% and 16% respectively.
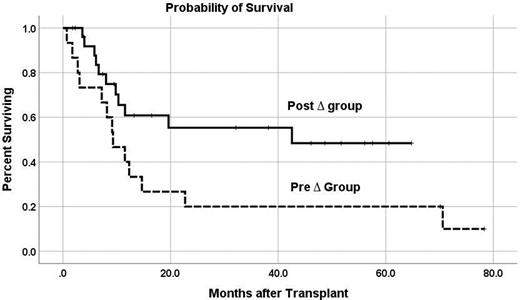
Fifteen patients (36%)-"Pre∆ group", were treated from 2013-2014 and twenty seven patients (64%)-"Post ∆ group" were treated from 2015-2020. Univariate comparisons revealed no significant differences between the Pre∆ and Post∆ groups in terms of age (p=0.53), diagnoses (p=0.72) or Revised Disease Risk Index category (p=0.14). Median HCT-CI score was 3.0 vs 2.7 in the Pre∆ and Post∆ groups (p=0.21) respectively, and the median KPS in both groups was 90% (p=0.62). OS was 20% vs 55% in the Pre∆ and Post∆ groups (p=0.044), CI of relapse was 27% vs 20% (p=0.60) and CI of NRM was 53% vs 31% (p=0.34) respectively. CI of acute GVHD and chronic GVHD was 33% vs 51% (p=0.41) and 20% vs 13% (p=0.92) in the Pre∆ and Post∆ groups respectively.
Conclusion: Haploidentical transplantation using the two-step T cell tolerization approach is feasible and encouraging in older patients. An adjusted risk model incorporating age, HCT-CI and KPS should be utilized in selecting older patients who are candidates for transplant.
Gergis:Incyte: Speakers Bureau; Merck: Speakers Bureau; Astellas: Consultancy, Speakers Bureau; Kite: Speakers Bureau; Mesoblast: Other: Ad Board; Jazz: Other: Ad board, Speakers Bureau. Flomenberg:Tevogen: Consultancy, Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal